
H. DIAGNOSIS
Wherever possible a louse comb should be used for the diagnosis of a head louse infestation. For this purpose, the hair should be first washed with a conditioner and after rinsing and while the hair is wet, a regular brush should be used to untangle the hair. A large light-colored towel could be place around the child’s shoulders during combing.
The louse comb should be drawn down from the roots to the ends of the hair with every stroke, while towards the end of the combing the comb should be directed towards the examining person to prevent lice falling from the comb. After each stroke, the teeth of the comb should be checked for living lice, which should be removed by wiping the comb with a wet tissue paper. Hairs should be combed thoroughly with the edge of the teeth lightly touching the scalp. The scalp should be examined section by section, when hair clips could be helpful in separating the examined part of the hair from the parts, which were not yet examined.
An examination with a louse comb for the period of 5 min, or at least 20 passes with a louse comb should be sufficiently effective in detecting lice. Long examinations could be painful for the child or cause him discomfort. If there is a suspicion that the child is infested with lice but no lice can be find during the examination, another occasion should be found to reexamine the child again.
EXAMINATION WITH A LOUSE COMB
The combing should be discontinued when the first louse is seen between the teeth of the comb. A magnifying glass and bright light may help to see, especially the young stages of lice.
Metal combs are more suitable than some plastic combs, which during use could produce static electricity and propel lice from the head of the infested individual to the examining person.
In case that the hair are long and in addition curly or frizzy, it is difficult and painful to use a louse comb. In these cases, the head should be examined visually by parting the hair every 2-3 cm and looking at the base of the hair for any moving louse. Due to the fact that this examination method is less effective in finding living lice, it should last for at least 10 min.
LICE ON THE SCALP
A child is diagnosed with a head louse infestation if a living louse is found on the scalp. Restriction of the term ‘nit’ to the empty eggshell, as distinct from the non-hatched egg, has been encouraged for many years. Non-hatched eggs could be either dead, e.g., due to a previous treatment, or alive. It is generally acknowledged that it is very difficult to distinguish viable from non-viable eggs with the naked eye.
Nits (empty eggshells) may remain attached to the hair for up to 8 months. Nits are mat, collapsed and white in color.
Fig. 4. Mumcuoglu
Though louse eggs are laid on the base of the hair, usually 3 mm from the skin, the nits which remain behind after the new louse left the egg, move away from the scalp as the human hair grows at a rate of about 1 cm per month (Fig. 4). After 2–3 months, the nits are more visible on the surface, particularly on dark hair (Fig. 5). The appearance of “eggs” several months after the last treatment can lead to a false positive diagnosis of infestation, as most people assume that if eggs are present the child must also have lice. In general, louse eggs found more than 0.5 mm from the scalp are unlikely to be viable (14, 15, 16).

Fig. 4. Mumcuoglu
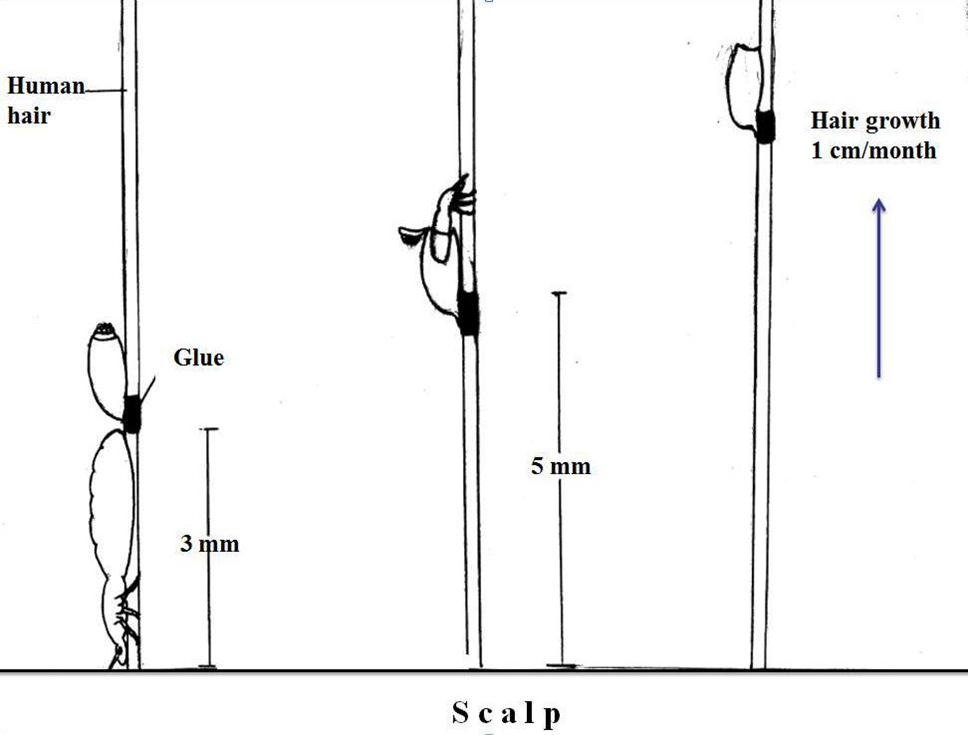
Fig.5. Mumcuoglu
Accordingly, when the diagnosis of head louse infestation is based on the presence of nits, 1–2 out of 3 children will be treated without justification. Pediculicides will not eliminate nits. Therefore, there would be no change in the appearance of nits on a scalp after an effective pediculicidal treatment. The presence of nits alone is thus interpreted as treatment failure and “infested” individuals continue to be treated unnecessarily.
Accordingly, if no living lice are detected using an accurate method of detection, the child or adult should be considered negative for head louse infestation. Nobody should be treated with a pediculicide unless living lice were found on the scalp.
Children who scratch their head continuously, those who supposedly come in contact with other presumably head-louse infested children or those who have nits on their heads, should be examined with a louse comb for few consecutive days and then one week later for living lice. It was shown, that children with nits are usually at higher risk of a new infestation than children that have not been infested in the last 2-5 months, i.e., children without nits (17).
Many examinations for head lice are being done by direct visual examination by hand, and the diagnosis of louse infestation is mainly based on the presence of nits. Combing the hair with a louse comb is 4-5 times more effective in the diagnosis of a louse infestation, and twice as fast as examination by hand (16, 18).
Direct visual examination therefore commonly underestimates active infestation. It is particularly difficult to diagnose a louse infestation accurately by hand examination, since approximately 78% of the infested children have only 1–10 lice on their scalp, 18.7% had 11–20 lice and only 3.3% had over 20 lice (10). Most of the lice on the scalp are nymphs, 1-2 mm in length, and therefore difficult to see without a magnifying glass. In addition, direct visual examination reveals a higher percentage of children with nits only than the examination with a comb, as the examining person spend more time looking at the hair rather than at the comb. Therefore, the chances of diagnosing a false-positive infestation are greater when examining by hand, and even more so, if the examiner is experienced in finding nits.
In those children with long and/or curly and frizzy hair, where the use of a comb on dry hair is very difficult, the inspection could be done either by direct visual examination or by treating the hair with conditioner, opening the nods with the help of a regular brush or comb and using a louse comb thereafter. As the detection of lice in long and curly/frizzy hair is more difficult, the examination should last longer.
When a member of the family is found to be infested, all other family members, especially young children and their mothers, should be examined and only those infested should be treated.